Physical Examination : The Perineum and Genital Examinations
Examination of the genitalia should occur within the context of a complete physical exam. Children generally respond well to this part of the examination when the examiner is confident, uses age-appropriate language to explain what is happening, and can find ways to engage the child.
Using a Colposcope
If available, a colposcope should be utilized by a trained examiner. The advantages of a colposcope include provision of a focused light source, magnification of the external anatomy, and the opportunity to record the findings of the examinations using an attached camera. If children are given the opportunity to see the colposcope prior to the examination, its use is more likely to be nonthreatening. Note that children and parents should be made aware that the colposcope is not used invasively (external only), and its main purpose is for examination and potential use for documentation of findings. Colposcope cameras may allow digital images to be transferred to secure storage, including still or video-recordings. For additional information regarding video versus still imaging, see Killough et al. If no colposcope is available, a light source such as the light from an otoscope may be helpful, although the magnification provided is limited. For more information see DOCUMENTATION: Photographic Documentation.
Positioning
The supine position is most commonly used in genital exams, particularly in the pre-adolescent population. Depending on the comfort of the patient, various positions may be utilized. Note that children/adolescents may have been abused in one or more of these positions and care should be taken to avoid retraumatization through use of an examination position. These include:
- The supine lithotomy position with stirrups
- The supine frog leg position on the parent's lap or exam table.
- The prone knee chest position
- The lateral knee chest position (lateral decubitus)
- Standing, leaning over the examination table
The prone knee-chest position is not commonly utilized but may be used if needed to improve visualization of the posterior hymen, perineal and anal areas. When using the prone knee chest position, the medical provider and assistant should guide the child into the position and provide constant reassurance. The prone-knee chest may be especially uncomfortable, as it is difficult for the patient to have a view of the examiner in this position.
Inspection/Palpation of the Genitalia
If photos are not obtained, document the findings of the anal/genital region on anatomical drawings, noting location and the explanation offered for any lesions found. If photos are obtained, the narrative documentation should correspond to and explain any findings. Always document the exam position when indicating findings. A superimposed clock face may assist in accurate documentation for females (Figure A). Conventionally, "12 o'clock" is anterior.
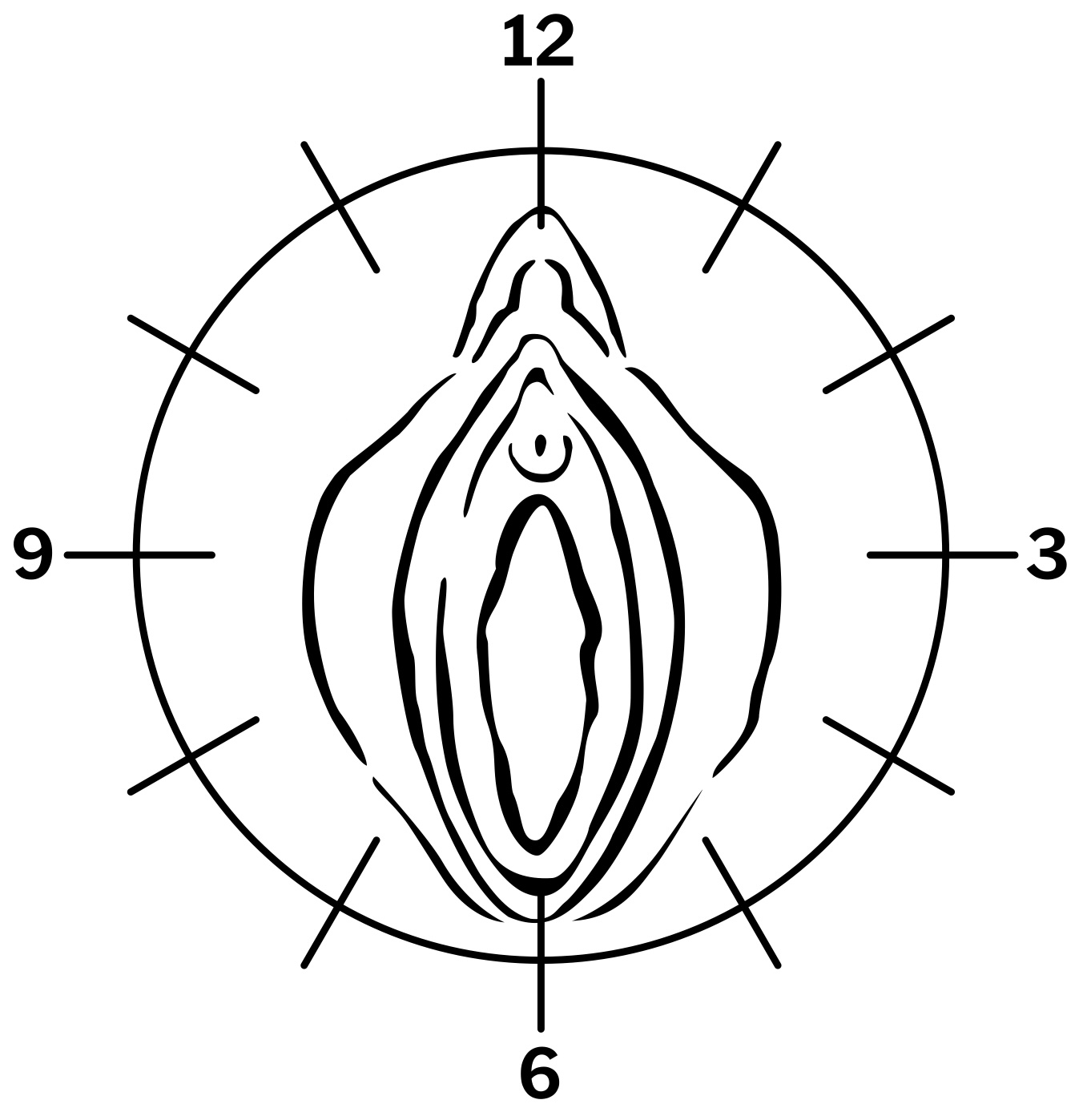
Figure A: Clock face superimposed on female genital area
Sabra Snyder, State University of New York, Upstate Medical University Medical Photography and Graphics
Note, if within 96 hours of the sexual assault, examine for dried or moist secretions. The following areas should be assessed:
- Pubic hair development
- Estimate the Tanner stage. For more information about Tanner staging, see Bright Futures curriculum for pediatric providers: https://www.brightfutures.org/wellchildcare/toolkit/maturity.htm.
- Inguinal adenopathy
- Check for redness, tenderness, if fixed or mobile, and size. Estimate node diameter, if enlarged.
- Medial aspects of the thigh
- Ecchymotic grab marks, bite marks, or for evidence of other injuries. Note any healed scars, STI lesions, or other abnormal findings.
- Perineum
- Note the presence of any fresh or healed lacerations, STI lesions, pubic lice, rashes, or other unusual findings.
- Vaginal or urethral discharge
- Note presence of discharge in terms of amount, color, and presence of odor. Identify the source, the vagina or urethra.
- Sexually transmitted infections
- Note presence of condyloma acuminata, condyloma lata, herpes, or primary syphilis lesions. For information on STIs see: LABORATORY: Testing for Sexually Transmitted Infections in Children and Adolescents and the CDC website: https://www.cdc.gov/std/treatment-guidelines/.
Female Genital Examination
The genital examination of the prepubertal child is principally external visualization. Instrumentation, such as use of a speculum is rarely, if ever, necessary for children or adolescents. All visualization and photography should be completed before attempting any specimen collection. If the use of a speculum in an adolescent is required, for example if there is a concern for a lesion in the upper part of the vaginal wall, use the smallest size possible. Never use an adult size speculum to examine a prepubescent child.
Labial traction is a technique to assist in the examination of the female genitalia. This technique can be used to open the vaginal orifice to better inspect the vagina for trauma, foreign body, and discharge and the hymenal anatomy for tears, scars, and attenuation. To use the labial traction technique in the supine frog leg position, grasp the labia gently between the thumb and index finger of each hand, and exert gentle downward and lateral traction (Figure B). Do not insert fingers to determine the size of the hymenal opening or its patency. This is not only not recommended, it does not provide any useful information.
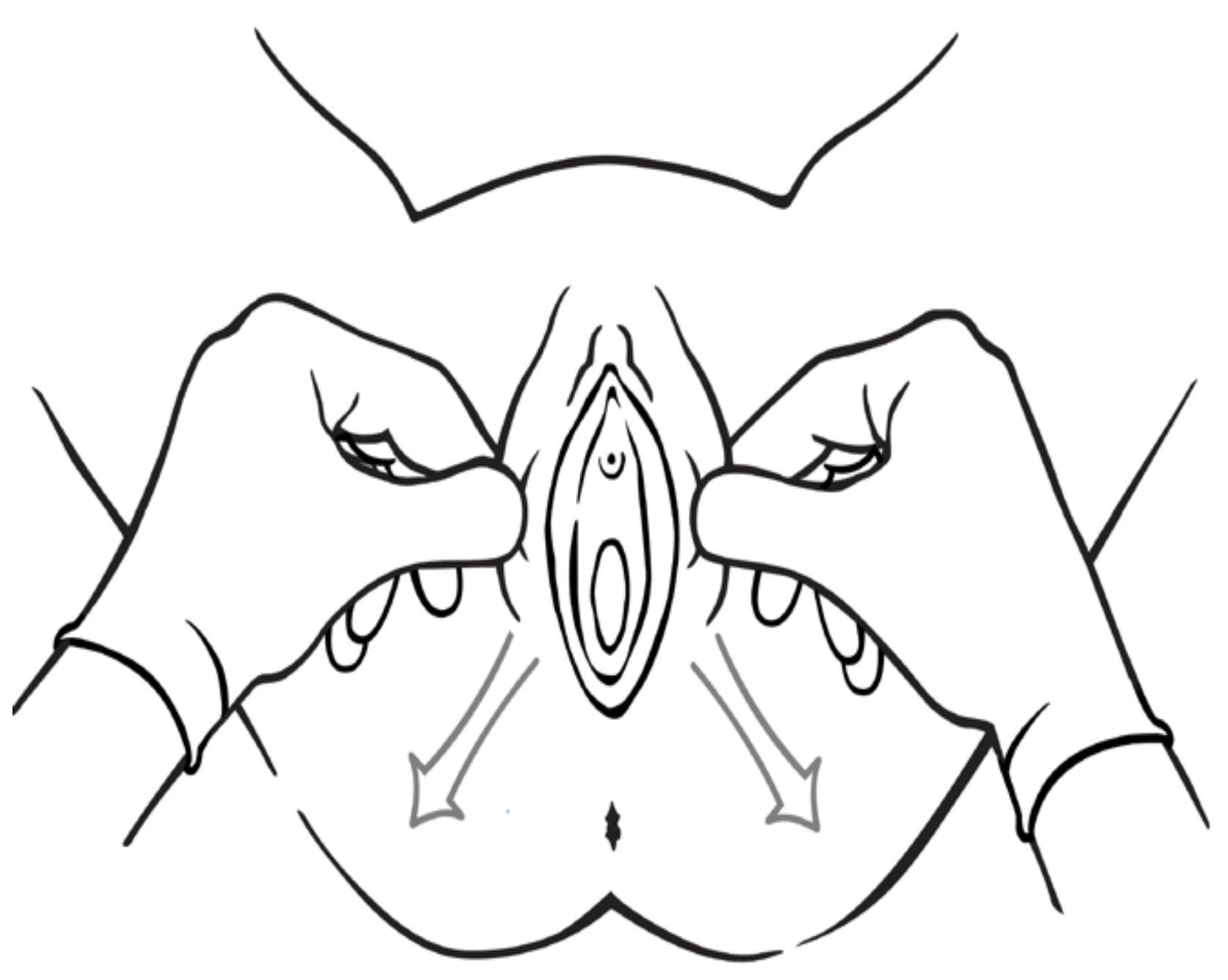
Figure B: Labial traction in the supine frog leg position
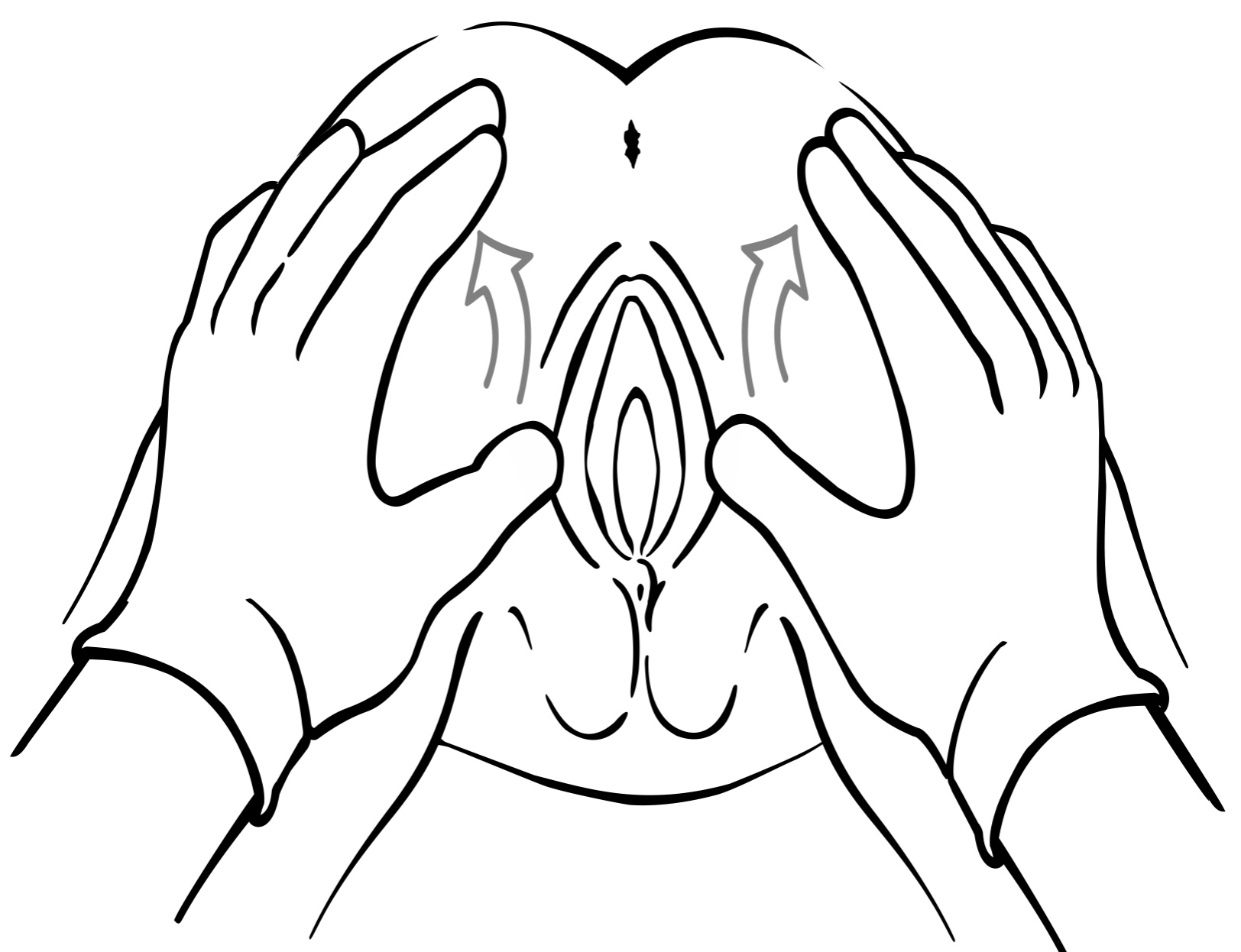
Figure C: Labial traction in the prone knee chest position
Sabra Snyder, State University of New York, Upstate Medical University Medical Photography and Graphics
When the child is in the prone knee chest position, separating the labia with both hands will display the hymen and vagina (Figure C). This position may give better visualization of the posterior rim of the hymen as it is pulled downward by gravity. If this causes such discomfort that the child is unable to cooperate, use another position. One alternative is to have the child lie supine, holding her knees to her chest.
Gently retract the labia majora to observe the genital structures. If the child is relaxed, the vagina and introitus will gradually open to reveal its maximum size. The size of the vaginal opening is affected by position and the degree of the relaxation/sedation of the child. For this reason, measurement of the transverse vaginal opening measurement is not recommended. Variation exists in the hymenal anatomy configuration among all children.
Examine the following:
- Labia majora and minora
- Note any skin changes, unusual pigmentations, or other skin lesions.
- Clitoris
- Note unusual size or changes of the clitoris or hood.
- Urethral meatus
- Note any signs of inflammation, edema, or other lesions of the periurethral tissue.
- Perihymenal tissue (vestibule)
- Note any increases in vascularity, erythema, abrasions, lacerations, scarring, or STI lesions.
- Hymen
- Note the configuration (annular, fimbriated, crescent) of the hymen in your narrative documentation. Observe for signs of trauma or STI lesions and document. Evaluate for fresh tears, transections, fresh hemorrhages, abrasions, and bruises. In addition, evaluate for ecchymotic areas, healed scars or adhesions, and abnormal vascular patterns. Hymenal abnormalities should be referred to a child abuse pediatrician or advanced practice provider with expertise for further examination or peer review of photographs. The terms "intact, broken, virginal, marital, or missing" are not appropriate to describe hymenal findings. If you are unsure of a finding, document the potential concern and area in question, and refer for further evaluation by an expert. Do not attempt to interpret a finding if you are unsure.
- Posterior fourchette and fossa navicularis
- Note lacerations or scars, bruises, healing abraded areas, STI lesions, or neovascularization.
- Vagina
- Note any bleeding, discharge, STI lesions, foreign bodies, abnormal vascular pattern, petechiae, or other findings on the walls of the vagina.
- Cervix
- Note any bleeding, discharge, STI lesions, cervicitis, tears, or signs of trauma.
Consider participating in the online Maintenance of Certification course for Evaluating Child Sexual Abuse, with free registration for course (small fee for CME and MOC): https://www.champprogram.com/courses.php
Male Genital Examination
Examine the following:
- Penis
- Note whether patient is circumcised. Note any STI lesions, bite marks, edema, hematomas, lacerations, abrasions, or dried secretions.
- Urethral Meatus
- Note any scars, STI lesions, discharge, or bleeding.
- Scrotum
- Note any erythema, ecchymoses, STI lesions, abrasions, or bite marks.
- Testes
- Note the presence of descended testes, any signs of atrophy or differential in firmness of the tissue.
Note testicle size, scrotum, and phallus development to assess Tanner stage. For more information about Tanner staging, see Bright Futures curriculum for pediatric providers: https://www.brightfutures.org/wellchildcare/toolkit/maturity.html
Anal/Rectal Examination
With either the supine or prone knee-chest position, the examiner should use both hands to separate the buttocks for viewing of the anal area in males or females. In general, traction techniques are not necessary when these positions are used. Note in the medical record the exam position that is utilized.
Examine the following:
- Buttocks
- Note fresh or healed tears, dried secretions, ecchymoses, rashes, STI lesions, bruises in the shape of a hand, fingers, or other patterned bruise.
- Perianal skin
- Examine for presence of inflammation. Record findings of dried secretions, bruising, tears, lacerations, fissures, tears, or lacerations that are located on the external surface, internal to the sphincter, or extend across the pectinate line, which is the juncture between the anal mucosa and the anal epithelium.
- Anal
- Note whether the verge or anal sphincter skin folds appear to be normal or abnormal in size or shape.
- A visual examination is sufficient to assess anal tone. Avoid a digital rectal examination in children unless there is suspicion of internal trauma.
- Apply only enough lateral traction to separate the buttocks. Dilation of the anus should be documented, however the significance of this finding in children is uncertain. Record the presence or absence of stool in the rectal ampulla.
- Rectal examination
- A rectal examination is rarely necessary in the evaluation of sexual abuse, even when there is evidence of trauma to the rectum. In situations where significant intraabdominal or rectal trauma is suspected, or when the presence of a foreign body is suspected, a digital examination may be justified. Consider further evaluation utilizing anoscopy and possible sedation.